



Inside Addiction: What I Wish You Knew
Part 1 of a series on recovery, science, and living with addiction.


My choice to be open about being in recovery from addiction isn’t so much about inspiring others to follow the same path as me. It’s not really about helping people feel less alone. It’s not about accruing followers or pity.
It’s about getting people to take a look into a world they may not understand.
It’s about showing people who have influence, power and money that this is a disease, and people do not wake up one day and choose to become an addict. It’s about explaining that this is a serious, and so often fatal, disease. It’s chronic, incurable, and something addicts have to monitor and treat every single day.
I always wanted Trainwrecks to be a place where I could share these thoughts, but it’s terrifying to pull the trigger on being explicitly honest about being an addict, because of the very real stigma. But I feel that being open gives these stories more power. As someone with a master’s in writing and lived experience, I think these words carry more weight — and I’m in a fairly unique position to communicate what people suffering from addiction actually experience.

I was 23 when I first went into alcohol and drug treatment. I remember it so vividly. My friend dropped me at the door of an outpatient AOD programme. I was scared, and so ashamed of needing to be there. I was also too young to comprehend the seriousness of the disease, so I continued to run my catering business and go to F45—I thought these things made up for failing in recovery.
I went to that building three or four times a week and sat there for three hours every time. And every week, I relapsed. It was insane. It took seven more years of living in this cycle—where things got a lot worse—before I finally got it.

I have a background in the sciences (I have a BSc from Otago), and it taught me the importance of understand the mechanisms of how something works—why it is the way it is, and what causes an outcome, behaviour or process. So I want to start this series off with why addiction is a disease, as it’s something I didn’t really understand until I went into treatment. I always thought I was a weak or bad person when I couldn’t stop using substances. It was honestly baffling—to so desperately want to stop, and then fail every single day.
“people jeopardize their lives for the sake of making the moment livable. Nothing sways them from the habit—not illness, not the sacrifice of love and relationship, not the loss of all earthly goods, not the crushing of their dignity, not the fear of dying. The drive is that relentless.”
― Gabor Maté, In the Realm of Hungry Ghosts
A disease is a condition that disrupts how the body or mind normally functions, has identifiable symptoms, and is caused by underlying biological or physiological changes. Here’s a simple breakdown of how addiction meets this criteria:
Addiction as a Disease: A Simple Breakdown
1. The organ involved:
Addiction is a disease of the brain. Just like asthma affects the lungs or diabetes affects the pancreas, addiction disrupts how the brain works.
2. The fault in the organ:
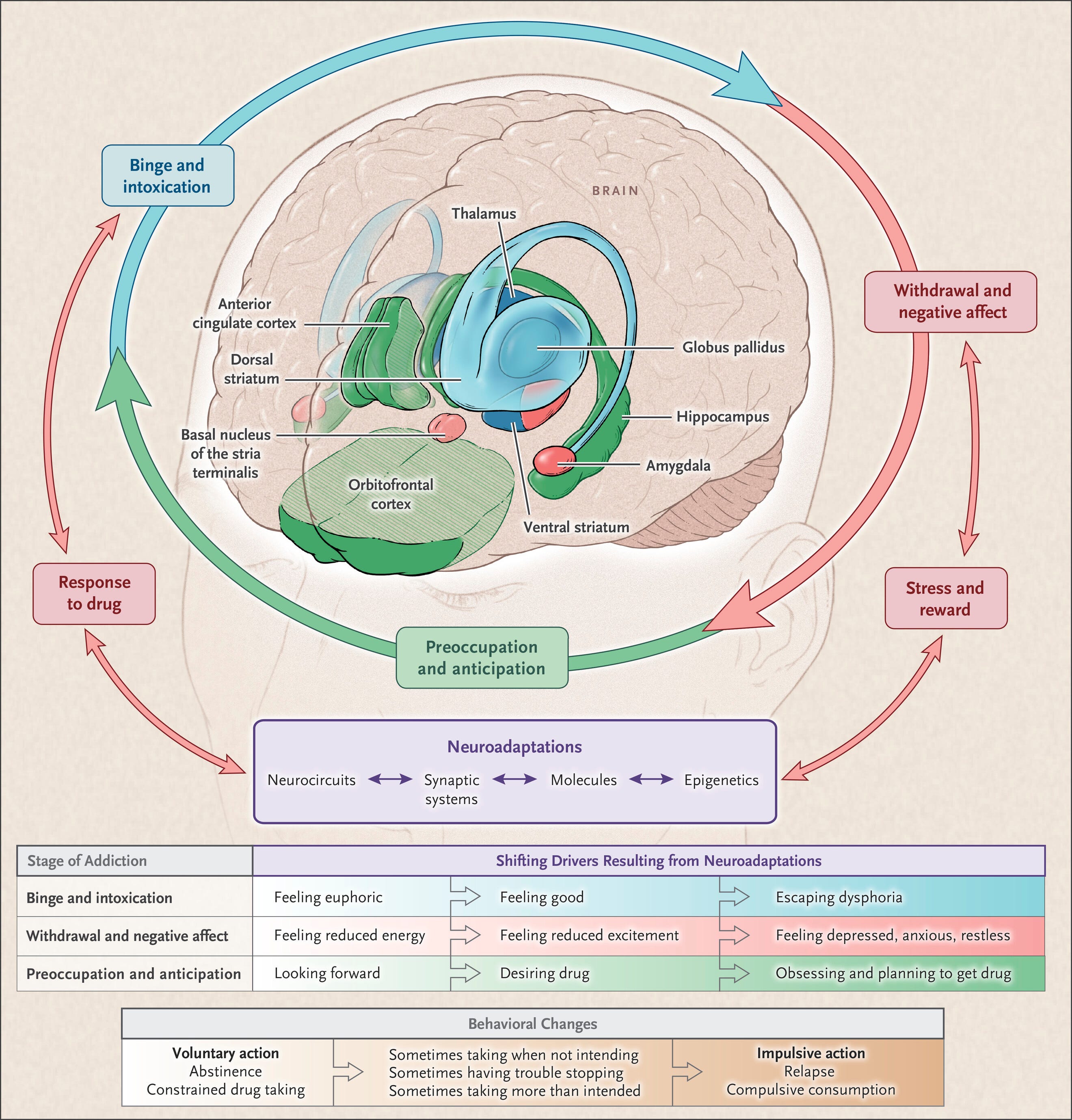
In addiction, the brain’s reward system gets hijacked. Normally, this system helps us survive—it rewards things like eating, social connection, and exercise by releasing dopamine, a chemical that makes us feel good.
But drugs and addictive behaviours flood the brain with dopamine in ways natural things don’t. Over time, the brain adjusts—it starts needing more and more of the substance or behaviour just to feel normal. It also becomes less sensitive to natural rewards.
This rewiring affects key areas of the brain:
The prefrontal cortex (decision-making, self-control)
The amygdala (emotions, stress)
The nucleus accumbens (pleasure and motivation)
These changes are physical and measurable—brain scans show differences in people with addiction.
3. The symptoms that result:
Because of these brain changes, people with addiction:
Crave the substance intensely
Lose control over their use, even when they want to stop
Keep using despite harm—much like someone with a damaged pancreas keeps having blood sugar issues
In other words: the faulty organ (brain) produces symptoms (craving, compulsive use, relapse)—which is how diseases work.
4. Not just bad choices:
Addiction often starts with a choice (like trying a drug), but so do many diseases. Smoking can cause lung disease. Poor diet can lead to heart disease. Once the disease is established, choice has far less power—because the organ itself has changed.

I really hope you’ve got something from this newsletter. It’s truly my hope that you’ve gained a new level of empathy or understanding for the portion of our society suffering from this disease.
"Don't ask why the addiction, ask why the pain. To understand people's pain, you have to understand their lives".
― Gabor Maté
As always, feel free to respond or ask any questions—and thank you for subscribing and reading. It would mean the world if you could share this with anyone you think might be interested. I’m going to go into more personal details as this series goes on, so if there’s anything you want me to cover, please let me know.
xx
Sources used in this article:
Blum, K., Werner, T., Carnes, S., Carnes, P., Bowirrat, A., Giordano, J. & Gold, M., 2023. Neurobiology of Addiction. StatPearls Publishing [Accessed 3 Jun. 2025].
Koob, G.F. & Volkow, N.D., 2016. The neurobiology of addiction: a neurocircuitry analysis. The Lancet Psychiatry, 3(8), pp.760–773. Read [Accessed 3 Jun. 2025].
Leshner, A.I., 1997. Addiction is a brain disease, and it matters. Science, 278(5335), pp.45–47. Read [Accessed 3 Jun. 2025].
Volkow, N.D., Koob, G.F. & McLellan, A.T., 2016. Neurobiologic advances from the brain disease model of addiction. The New England Journal of Medicine, 374(4), pp.363–371. Read [Accessed 3 Jun. 2025].
Volkow, N.D. & Koob, G.F., 2021. Addiction as a brain disease revised: why it still matters, and the need for consilience. Neuropsychopharmacology, 46, pp.1715–1721. Read [Accessed 3 Jun. 2025].
There are many ‘sober’ people who still believe that addiction often originates from a bout of boredom or simple recklessness, where a person consumed recreationally but became heavily hooked on a substance that eventually destroyed their life and by extension even the lives of loved-ones.
In the book (WHAT HAPPENED TO YOU?: Conversations on Trauma, Resilience and Healing) he co-authored with Oprah Winfrey, Dr. Bruce D. Perry (M.D., Ph.D.) writes in regards to self-medicating trauma, substance abuse and addiction:
“But here’s what’s interesting about drug use: For people who are pretty well-regulated, whose basic needs have been met, who have other healthy forms of reward, taking a drug will have some impact, but the pull to come back and use again and again is not as powerful. It may be a pleasurable feeling, but you’re not necessarily going to become addicted.
“Addiction is complex. But I believe that many people who struggle with drug and alcohol abuse are actually trying to self-medicate due to their developmental histories of adversity and trauma.”
Decades ago, I, while always sympathetic, also looked down on those who had ‘allowed’ themselves to become addicted to hard drugs or alcohol. Although I’ve not been personally or familially affected by the opioid overdose crisis, I have suffered enough unrelenting PTSD symptoms to have known, enjoyed and appreciated the great release upon consuming alcohol or THC.
The unfortunate fact about self-medicating is: the greater the induced euphoria or escape one attains from it, the more one wants to repeat the experience; and the more intolerable one finds their non-self-medicating reality, the more pleasurable that escape will likely be perceived. In other words: the greater one’s mental pain or trauma while not self-medicating, the greater the need for escape from one's reality — all the more addictive the euphoric escape-form will likely be.
When substance abuse is due to past formidable mental trauma, the lasting solitarily-suffered turmoil can readily make each day an ordeal unless the traumatized mind is medicated. Not surprising, many chronically addicted people won’t miss this world if they never wake up.
Regardless, societally neglecting, rejecting and therefore failing people struggling with crippling addiction should never be an acceptable or preferable political, economic or religious/morality option. They definitely should not be consciously or subconsciously perceived by sober society as somehow being disposable. Too often the worth(lessness) of the substance abuser is measured basically by their ‘productivity’ or lack thereof. They may then begin perceiving themselves as worthless and accordingly live and self-medicate their daily lives more haphazardly.
Meantime, substance abuse, addictions and addicts are still largely perceived by ‘sober’ society as being products of weak willpower and/or moral crime. At the same time, pharmaceutical corporations have intentionally pushed their own very addictive and profitable opiate resulting in immense suffering and overdose death numbers — indeed the real moral crime! — and got off relatively lightly and only through civil litigation.
So, so, so proud of you! Thanks for sharing your story.